
Are we sleepwalking into another pandemic?
As the H5N1 bird flu virus infects more and more mammalian species, including cattle and humans, the danger of a pandemic is growing. So when will we wake up to the 'monster at our door'?

Five years ago this month, public health experts began hearing reports of a mysterious pneumonia in Wuhan. At the time, few people outside of China had heard of Wuhan and with the world’s eyes focussed on the bush fires in southern Australia, the reports barely rated a mention in the media. Even when on January 12, China’s Centre for Disease Control announced that the pneumonias were due to a novel coronavirus and released the virus’s genetic code, few people outside of scientific circles took notice.
We all know what happened next. Spreading rapidly from China to Southeast Asia, North America, Europe and Africa, Covid-19 would claim more than 20 million lives worldwide and trigger a series of lockdowns unprecedented in peacetime. Those lockdowns were necessary because, despite the examples of the 2002 SARS epidemic – also due to a coronavirus - and the 2009 swine fu pandemic, few governments had thought through what might be required to contain a high consequence respiratory pathogen against which there was no vaccine and with the potential to wipe trillions of dollars off the global economy.
The question today is are we sleepwalking into another pandemic?
It cannot have escaped your attention that we are in the midst of the worst flu season since the winter of 2022/23, with the UK seeing a staggering 5,000 hospital admissions this past December, four times as many as in November. If your New Year’s Eve was anything like mine, it was marked by vacant chairs and friends coughing and spluttering in the corner. Though Covid-19 cases are down compared to previous years and the tabloid talk of a “Quademic” of flu, Covid-19, RSV and norovirus has yet to materialise, it has been grim holiday season with the head of the Royal College of Emergency Medicine telling the BBC that pressures on hospitals are “unacceptably awful” and that services are at breaking point. Adding to the sense of deja vu is a worrying surge in respiratory infections in China over the same period.1
But these concerns pale into comparison with what the medical sociologist Mike Davis once called the “monster at our door”. Davis, who died two years ago, was referring to avian influenza – in particular, the H5N1 strain of the bird flu virus that first emerged in Guangdong in southern China in 1997 and which, by 2005, was causing outbreaks across Southeast Asia, prompting the mass culling of poultry.
As reports over the holiday period make clear, the threat has not gone away. If anything, the alarm bells are ringing louder than ever.
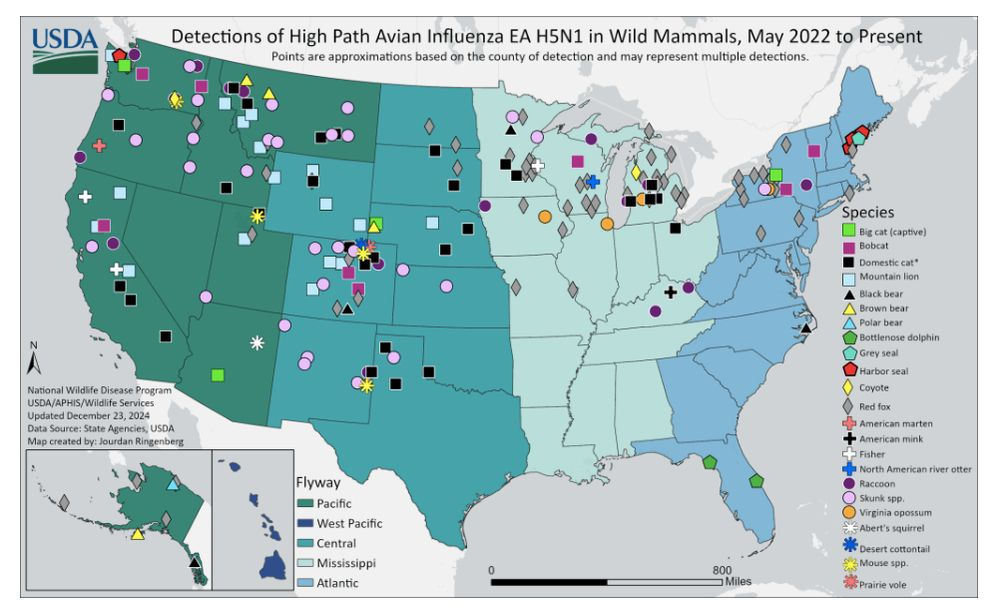
Since 1997, H5N1 has been isolated from wild bird populations on every continent except Australia. In recent years, the virus has also been detected in a range of mammals, including seals, Sea lions, mink, skunks and racoon dogs. Even more worrying is the infection of US dairy cattle. Since March 2024, the virus has been detected in cattle herds in16 US states. There have also been 66 confirmed and 8 probable human cases (the cases are due to either the H5N1 type circulating in birds, known as clade 2.3.4.4b, genotype D1.1, or the genotype circulating in dairy cows: B3.13).
The most alarming case of all is that of a 13-year-old Canadian girl from Vancouver. According to a recent report in the New England Journal of Medicine, the girl initially presented with conjunctivitis and fever on November 4 and was sent home without treatment. But three days later she developed respiratory distress, prompting her to be admitted to British Colombia Children’s Hospital. There, in scenes reminiscent of the first months of Covid-19, she was admitted to the hospital’s ICU, intubated and placed on an ECMO machine.
The pathology was truly terrifying. By day five, a scan of her left lung showed it was occluded with fluids and damaged cells consistent with viral pneumonia. She also required dialysis for kidney failure. Fortunately, the infection responded to treatment with antiviral medications. Nonetheless, the girl spent two weeks on ECMO and almost three weeks on a ventilator, prompting the hospital to issue nursing staff with N95 respirators and eyeglasses to prevent droplet and aerosol infection. Tests subsequently revealed the girl’s symptoms were due to the same type of H5N1 that is circulating in wild birds. Most worrying of all, the virus showed adaptation to sialic acid receptors in the human respiratory tract.

There could hardly be a clearer example of the need for continued vigilance against H5N1 and other highly pathogenic respiratory viruses, including Covid-19. But as WHO epidemiologist Maria Van Kerkhove complained at a recent conference in Japan: “Everyone is acting as though this pandemic [of Covid-19] didn’t really happen.”
The virologist Angie Rasmussen puts it even more starkly. Complaining that the US’s response to the outbreak of H5N1 in dairy herds has been “awful”, she says that authorities urgently need to ramp up tests on cattle and dairy workers to get a better sense of how the virus is spreading and the extent to which it has contaminated America’s milk supply. Unless something changes soon, she warns, it is only a matter of time before we see more cases like the Canadian one.
“I get a lot of ‘lessons learned’ questions,” she tweeted recently. “My answer is ‘none”. We didn’t learn anything.”
While, so far, most human cases have not been as severe as the girl hospitalized in British Colombia, the virus has an average 50 percent fatality rate and Rasmussen warns that the D1.1 type has the potential to be as bad as other H5N1s. “At population scale, even infrequently, this is millions of people,” she warns.
All this as negotiations at the World Health Organization over a new pandemic agreement, that would see countries sharing information about emerging infectious disease threats in exchange for access to treatments and vaccines, have stalled and as the US prepares to inaugurate a new president hostile to science. Little wonder that ahead of Donald Trump’s return to the White House, Joe Biden has just committed an additional $306 million to tackling bird flu and will distribute the money before the 47th president takes office.
The good news is that the US and other countries, including the UK, have stockpiled H5N1 vaccines. Although these date back several years, they appear to be a good match for current strains, neutralizing the viruses in laboratory tests. However, it is anyone’s guess how well they will work in the real world.
In the event of an H5N1 pandemic, we could also deploy the latest mRNA vaccine technologies, as we did during Covid-19. Scientists at the US Centers for Disease Control and Prevention (CDC) recently reported that a prototype vaccine tested on ferrets, which have similar respiratory receptors to humans, enabled them to survive a lethal dose of H5N1. The bad news is that Trump’s nominee to head the Department of Health and Human Services, Robert F. Kennedy Jr, is an anti-vaxxer with a record of promoting quack cures for viral diseases. On taking office, Kennedy has also threatened to repeal legislation indemnifying vaccine manufacturers against claims for vaccine damage – a move that would make it harder to persuade pharmaceutical companies to invest in emergency vaccines.
But perhaps the biggest impediment is societal amnesia. Three years on from the height of the Covid waves, there is little public appetite for reflecting on our collective trauma and how best to prevent the re-occurrence of death on such a scale. Instead, it seems, we would rather forget the scenes of patients being intubated in hospital corridors and the endless lockdown days and nights that followed.
There are several reasons for this, which I have written about before. But if we take anything from the recent reports about bird flu it is that it is time to awaken from our slumbers.
The monster has been lurking at our door for many years now. It may not be prepared to wait much longer.
Note: as this article was going to press, the US Centers for Disease Control and Prevention (CDC) reported that a 65-year-old patient from Louisana died after being hospitalized with the D1.1 genotype apparently contracted from a backyard flock. Worryingly, one of the mutations that enabled the virus to infect the patent was identical to one detected in the girl from British Colombia. According to the CDC, the mutations were not present in virus samples taken from the backyard flock, suggesting that they developed in the pateint as the patient’s illness progressed. So far, there is no evidence that the mutated virus is able to spread efficiently between people but the worry is that should someone be simultaneously infected with the H5N1 virus and a seasonal flu, then it might recombine so as to spread efficiently among humans.
Thankfully, most of the infections are due to the human metapneumovirus (HMPV), a common respiratory virus similar to RSV that circulates all year round but which tends to be more prevalent at times of cold weather.